Patients were walking out.
Nobody knew exactly why.
The two VCU Health EDs involved in this project knew they had a walk-out problem. What they didn't have was a clear picture of what was driving it — or what changes would actually help. The standard assumption was that wait times were the culprit. The research told a more complicated story.

Listening to everyone
in the room.
As a team, we conducted 18 semi-structured interviews across both hospitals — emergency department technicians, nurses, all the way up to hospital presidents (who I personally interviewed) — then spent time in the waiting rooms observing directly: how people moved through the space, where communication broke down, what patients did when no one came to update them.
Staff and patient surveys ran in parallel to capture perceptions at scale and bring people into the design process early. Four themes emerged from the synthesis:
Between patients and staff — updates were rare, unclear, or delivered in open earshot of others
Internal handoffs were inconsistent, creating gaps that slowed care and compounded wait times
Waiting areas didn't support comfort or privacy — small stressors that amplified anxiety over time
Patients unfamiliar with how EDs work didn't know if their wait was normal — and assumed the worst
It wasn't the wait.
It was the not knowing.
After affinity mapping with the team, two challenges rose to the top — both about information, not time.
Patients felt unseen from the moment they arrived
No one was actively watching the waiting room. Triage conversations happened in open earshot. Patients tracked each other's conditions because no one was tracking theirs.
Getting a status update was nearly impossible
Patients couldn't easily reach the triage nurse — some asked the security guard. The uncertainty of not knowing was what pushed people out the door, not the wait itself.
.jpg)
Solutions from the people
who know the space best.
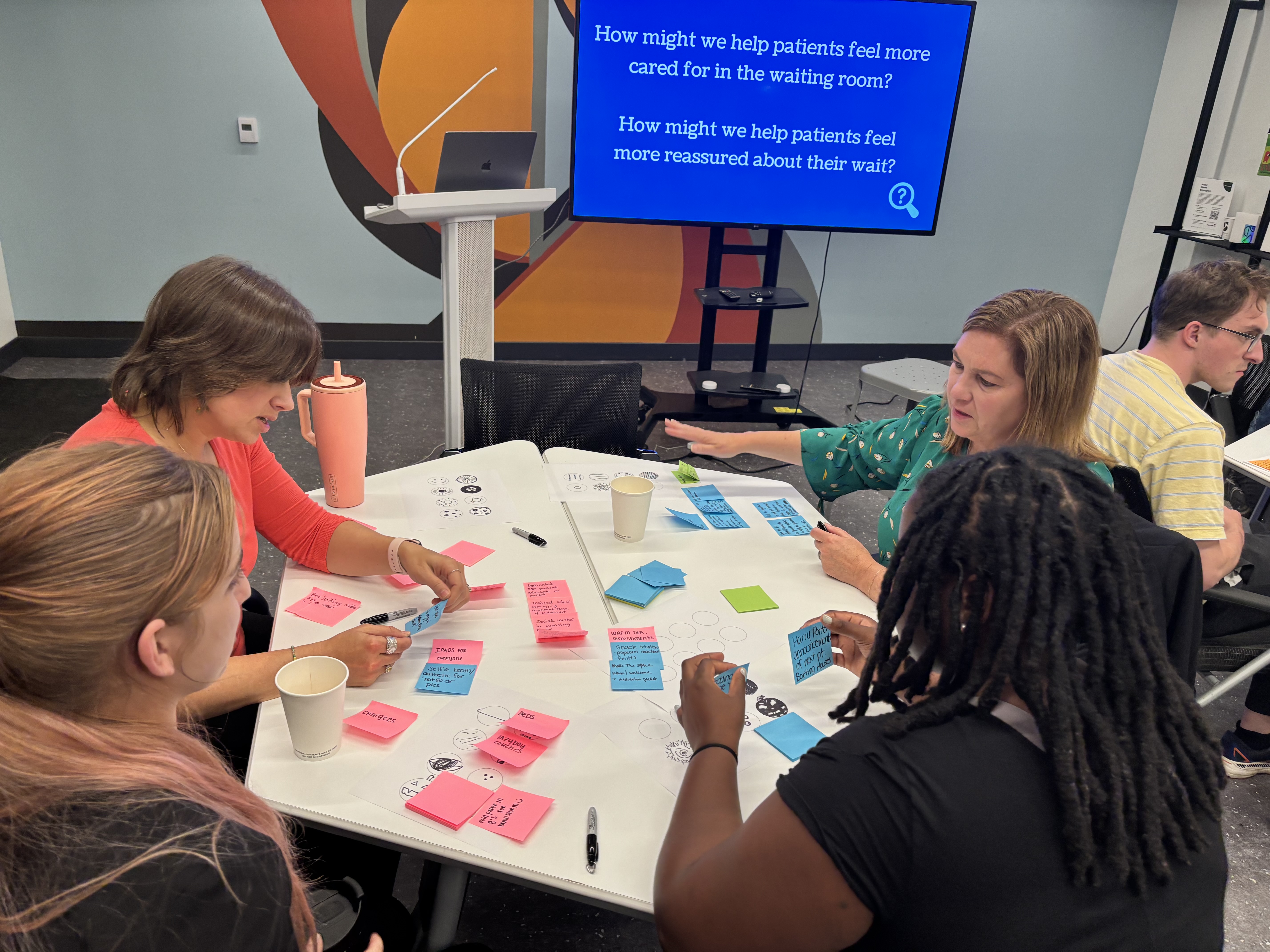
I co-facilitated workshops with frontline staff and providers that built on our research artifacts, guiding ideation through rapid brainstorming and dot voting to surface ideas that would actually work in practice. Four concepts emerged, ranging from a real-time patient status app (think: Domino's tracker for your ER wait) to a dedicated outdoor space for patients and staff to decompress. Each addressed the same underlying problem: helping patients feel held, informed, and cared for while they wait.
Real changes at
real hospitals.
The project closed with a demo day for hospital leadership. The response went beyond acknowledgment — the hospitals changed their hiring plans to add a nighttime physician, a direct result of findings about after-hours coverage gaps. Walk-outs dropped 50%, translating to an estimated $622k in annual savings.
The bigger lesson: when you give frontline workers a structured way to name what they're seeing and put leadership in the room to hear it, research becomes a conversation rather than a report. That's when things actually change.
"The process opened up conversations between frontline staff and leadership that hadn't happened before."— Project reflection, VCU Health Emergency Department initiative